On the 4th of February 2015, Dr Caroline Leaf gave her debut TED presentation, at TEDx Oakes Christian School, California.
Most TED watchers wouldn’t have heard of her before, but Caroline Leaf is a well-known name in western Christendom. She has spoken from pulpits on every continent. She’s authored one of the best selling books in the Christian market and has her own TV show on cable in the US. She’s followed by more than one hundred thousand people on Facebook, and she’s even run her own conference, with another in the pipeline. She’s a mega-star in the Christian world.
So who is this woman with the stiletto-heels and slick presentation? What was her training and background? How did she make it to the TEDx stage?
This aim of this post is to provide some context and background for those in the TED universe who have seen Dr Leaf’s TEDx presentation, and want some more information in assessing her TEDx debut, and indeed, the global Caroline Leaf phenomenon.
This review will be in four main parts: first I will give some basic information on Dr Leaf, I will compare Dr Leaf’s claims in her TEDx presentation to her published research results and some basic neuroscience, and lastly I’ll outline Dr Leaf’s general work and it’s accuracy compared to current science.
- WHO IS DR LEAF?
Dr Caroline Leaf was born and raised in South Africa, where she completed her school education and went on to attain the following degrees:
- Bachelors of Science (Logopaedics) – University of Cape Town 1985
- Masters in Audiology and Speech Pathology – University of Pretoria 1990
- Doctor Philosophiae (Communication Pathology) – University of Pretoria 1997 (http://drleaf.com/assets/files/DrCarolineLeaf_CurriculumVitae1.pdf)
Officially, Dr Leaf is qualified as a communication pathologist (which is a specialized combination of Speech Pathology and Audiology – see also: http://www.hpcsa.co.za/Uploads/editor/UserFiles/downloads/speech/slh_education_training_insitutions.pdf)
Dr Leaf worked for a number of clinics and school boards as a communication pathologist in the few years following the completion of her PhD (http://drleaf.com/assets/files/DrCarolineLeaf_CurriculumVitae1.pdf).
Dr Leaf has written a number of articles for publication in minor journals (see http://drleaf.com/assets/files/DrCarolineLeaf_CurriculumVitae1.pdf). Three of her papers were published in a small Medline indexed journal, “The South African Journal of Communication Disorders”. These are:
- “Mind-Mapping approach (MMA): a culture and language “free” technique”, 1993 (http://www.ncbi.nlm.nih.gov/pubmed/8047932)
- “The development of a model for geodesic learning: the geodesic information processing model”, 1997 (http://www.ncbi.nlm.nih.gov/pubmed/9819969)
- “An alternative non-traditional approach to learning: the metacognitive-mapping approach”, 1998 (http://www.ncbi.nlm.nih.gov/pubmed/10472179)
The journal happened to be edited by her supervisor and co-author, Dr Brenda Louw (see http://www.debunkingdrleaf.com/goodies), though I’m sure the selection of her articles for this journal was purely on merit.
Dr Leaf states on a number of occasions that she is a “cognitive neuroscientist”, and “a scientific and Biblical expert in the power of the human mind”.

This is despite the fact that Dr Leaf:
- does not have formal qualifications in neuroscience,
- has not worked at a university as a neuroscientist,
- has not worked in any neuroscience research labs,
- has not published any papers in neuroscience journals, and
- has not had any formal theological training.
Given the weight of evidence, Dr Leaf would be better described as an academic speech pathologist and lay preacher rather than a cognitive neuroscientist.
- DR LEAF’S RESEARCH RESULTS
Throughout her TEDx presentation, Dr Leaf repeatedly made reference to the results of her own research, suggesting that her pioneering work resulted in radically improved outcomes for the students involved in her research, and that her work with students one-on-one and through teacher education profoundly changed the learning of every student in her various programs.
For example, she said, “Well her IQ was 100 before the accident, it was 120 after the accident. So here with holes in her brain, and brain damage, she changed … she actually increased her intelligence. Now I’m pretty convinced at this stage, cause I’ve been working … besides her I’ve been working with lots and lots of other patients, seeing the same thing, when these students applied their mind, their brain was changing, their academic results were changing.”
Later she stated, “I wasn’t sure if this was going to have the same impact cause until this point I’d been working one on one. Well I’m happy to tell you that we had the same kind of results … The minute that the teachers actually started applying the techniques, we altered the trend significantly.”
And also, “I stand up here saying this with conviction because I have seen this over and over and over in so many different circumstances … in this country I worked in Dallas for three years in charter schools, and we found the same thing happening.”
However, her published results differ significantly from her claims.
The first research that Dr Leaf spoke of was of the sixteen-year-old girl who was the victim of a motor vehicle accident. This particular girl was Dr Leaf’s prime patient. The case study of this patient was presented in Dr Leaf’s unpublished Masters thesis, and was discussed in more detail in Dr Leaf’s paper, “Mind-Mapping approach (MMA): a culture and language “free” technique” [1], though it should be noted that no statistics were published in this paper, and on the third page of the article, Dr Leaf admitted that the result could actually have been spontaneous recovery rather than her own intervention.
Dr Leaf did further work within a number of schools for her PhD research. Dr Leaf compared the academic results for three schools for the years 1991 and 1992 to the results for 1993, during which she introduced her mind mapping approach (MMA). Generally, the results for 1993 were better than the results for 1992, which seems to indicate that Dr Leaf’s MMA training was effective. However, the results from 1991 to 1992 were already improving without her input [2: p182]. The difference in average marks between 1991 and 1992 was 1.76%, while the difference between 1992 and 1993 (the introduction of Dr Leaf’s MMA) was only 2.19%. If Dr Leaf’s program really was the cause of that improvement, then her program only resulted in a 0.43% improvement on average.
I have reproduced Dr Leaf’s original graph of the average overall results obtained in her PhD study. While Dr Leaf’s original graph makes her data look spectacular, when appropriately rescaled, the data looks quite ordinary.
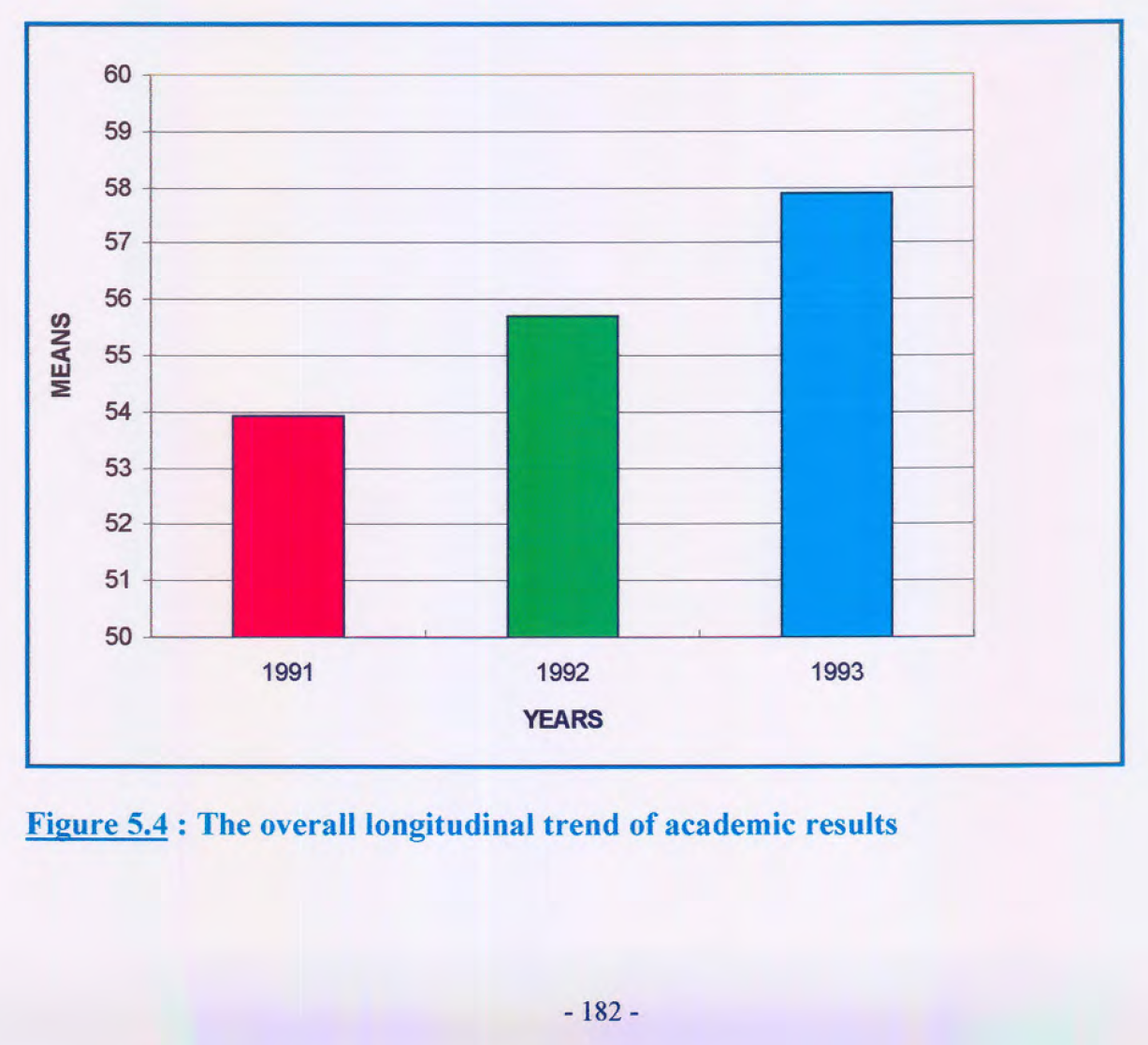

At best, Dr Leaf’s program gave the already positive momentum of the students a gentle nudge.
However, it should be noted that her program may have also hindered some students. Dr Leaf notes in her analysis: “The results obtained indicate that in general the academic trend in the three primary remedial schools was altered with the introduction of the MMA methods in 1993. Furthermore, it appears that the most positive response occurred in phase one (grades 1 and 2, standard 1). A positive response also occurred in phase two (standards 2-4) but this change was just outside the significance level. Phase three (standard 5), by contrast, experienced negative effects with the introduction of the MMA methods.” [2: p181]
So to summarise, according to Dr Leaf’s own data, there was no clear benefit derived from her MMA program.
Dr Leaf then discussed her work in a number of charter schools that she performed in Dallas. This was part of testing of a program called the Switch On Your Brain 5-step learning process.
Dr Leaf claims that, “The Switch On Your Brain with the 5-Step Learning Process® was assessed in a group of charter schools in the Dallas. The results showed that the students’ thinking, understanding and knowledge improved across the board. It was concluded that The Switch On Your Brain with the 5-Step Learning Process® positively changed the way the students and teachers thought and approached learning.” http://drleaf.com/about/dr-leafs-research/
However, there has been no independent research into Dr Leaf’s Switch On Your Brain learning program or even the Geodesic Information Processing Theory, the theory Dr Leaf devised and on which the Switch On Your Brain program is based.
Dr Leaf published her own internal research into the program on her website. The project was a two year program involving teachers and students at a group of four schools in the Advantage Academy group in Dallas, Texas. This involved working with more than 150 teachers and 2000 students.
Despite her glowing self-assessment, Dr Leaf’s own published numbers suggest that the program is ineffective, or quite possibly a hindrance. For example, the graph below demonstrates the qualitative analysis of “content mastery” (which the paper describes as a combination of knowledge and understanding) for reading across all grades from 3rd to 12th, compared with the results from the previous year before the Switch On Your Brain was implemented. Dr Leaf omits a basic statistical analysis, but just by looking at the similarity of the scores, these results are more likely to be a chance effect, except for the 12th grade, where the previous cohort of students increased dramatically, where as the Switch On Your Brain cohort got slightly worse.

Rather than blame her program, Dr Leaf simply shifts the blame to the teachers: “The few cases where we see drops can be linked to teacher knowledge, attitude and skills and is diagnostic.”
The full research paper that Dr Leaf published is available at http://drleaf.com/assets/files/Web-page-AA-research-project-1.pdf if you wish to review the results for yourself.
The ineffectiveness of Dr Leaf’s program may be for many reasons, but I believe one is that it is built on a theory that relies on mind-mapping. Dr Leaf renamed her version of mind-mapping “The Metacog”, though it’s clear from her early academic work [1] that the Metacog and the Geodesic Information Processing Model [3] were based on the work of Tony Buzan. Buzan’s concept of mind-mapping has been used across multiple professional fields [4] and remains a valuable resource for brainstorming or gathering thoughts in a visual way. However, modern research (including a controlled trial within a primary school classroom environment) shows that mind mapping is a poor tool for learning [5-8].
- DR LEAF’S IRONIC INSPIRATIONS
Dr Leaf openly contradicts herself throughout her presentation, failing to realise that the stories she shared of her own patients disproved her vacuous inspirational memes.
Our biology affects each and every one of us. Our mind is a function of our brain. Our mind is to our brain as our breath is to our lungs. Put simply, without our brain, we would have no thoughts. If the structure and function of specific networks in our brains are altered, this changes our thinking. This is confirmed in everyday life – when someone suffers a brain injury or a stroke and they sustain damage to their brain, they suddenly lose the function of some, or all of their mind or body. Trans-cranial Magnetic Stimulation, Trans-cranial Direct Current Stimulation, metabolic states, prescription medications, illicit drugs, or everyday drugs like caffeine or alcohol have all been proven to change the subjects mental state through changes to the function of their brain. Any suggestion that our brain does not control our mind is simply ludicrous.
Clearly then our biology does control our psychology. Real cognitive neuroscientists have shown that our stream of thought is simply a tiny fraction of our overall neural activity, a conscious glimpse of the brains overall function [9-11], like the tachometer is for the engine in your car. Thus, our mind does not change our brain at all. Rather, it is our brain’s directed activity causing the growth of new synaptic branches to support it, something which the brain does without the function of conscious thought from the time when we were embryos.
Dr Leaf actually confirms this fact through her stories of her brain injured patients. After all, if “the mind is separate from the brain but influencing the brain”, then how could those victims of acquired brain injury lose cognitive function after their injury? If it were true that “each and every one of us is not a victim of our biology. We are a victor over and above our biology. We control our brain, our brain does not control us”, then how could those people with damage to their brains from strokes suddenly lose function?
The fact that Dr Leaf’s patients lost their mental or cognitive function because of damage to their brains directly contradicts her insistence that our brain and our mind are separate, and that our brain does not control our mind.
- FUNDAMENTALS OF DR LEAF’S OTHER TEACHING
Considered altogether, Dr Leaf’s teaching boils down to a few fundamentals;
* Thought is the main driving force that controls every other aspect of our lives (and our physical world).
* We have full control over our thoughts.
* Thought causes stress.
* Stress is directly responsible for nearly all serious physical and mental illness.
* Therefore thought causes the vast majority of human disease, making thoughts toxic, and
* If toxic thoughts cause disease, “detoxing” thoughts will cure or prevent disease.
On first inspection, each individual postulate doesn’t seem so bad. However, when fully considered and taken to their natural conclusions, they veer into conjecture and pseudoscience, as evidenced by Dr Leaf’s published works and public appearances.
For example, Dr Leaf states in her books:
“Thoughts influence every decision, word, action and physical reaction we make.” [12: p13]
“Our mind is designed to control the body, of which the brain is a part, not the other way around. Matter does not control us; we control matter through our thinking and choosing.” [13: p33]
“DNA actually changes shape according to our thoughts.” [13: p35]
On Facebook and in interviews, this translates to:
“Our genetic makeup fluctuates by the minute based on what we are thinking and choosing.” 27/9/2014
“The toxic thoughts in our minds become physical baggage in our brain, which literally cause brain damage.” 5/12/2014, 27/10/2014 and 7/10/2014
“Your mind will adjust your body’s biology and behaviour to fit with your beliefs.” 21/6/2014
“SID ROTH: But when you told me that we could change our genes I wish every doctor in the world would understand this cutting edge research because, you know, you go to a doctor and say your cholesterol was high, and they say, well, exercise, change your diet, but it could be your genes and there’s nothing you can do, so take this medicine that will have a zillion side effects. But you say, according to the latest brain research, if you follow what Jesus said you can change your genes. That’s just so amazing.
DR. LEAF: I know. It is phenomenal. If you think of it, it’s logical too, Sid …”
http://youtu.be/Uhbt_XOZTdA?t=50s. Full transcript: http://donate.sidroth.org//site/DocServer/IS571Transcript_Leaf.pdf?docID=2941
Dr Leaf draws her erroneous conclusions from the poor interpretation of poor evidence. For example, one of Dr Leaf’s favourite factoids is her statement that “Research shows that 75 to 98 percent of mental, physical and behavioral illness comes from one’s thought life.” [13: p33] Dr Leaf’s sources for this statement include, among others, an article that not only doesn’t mention the figure she attributes to it, but also directly contradicts her fundamental premise [14], and the misleading paraphrasing of an already dubious quote from a pseudoscientific author [15].
Dr Leaf also has a number of pet theories which betray her preference for pseudoscience, the main one being her assertion that the heart is actually a mini-brain that has dedicated cognitive functions. For example, in her books, she says,
“Your heart is in constant communication with your brain and the rest of your body, checking the accuracy and integrity of your thought life. As you are about to make a decision, your heart pops in a quiet word of advice, well worth listening to, because when you listen to your heart, it secretes the ANF hormone that gives you a feeling of peace.” [12: p62, 13: p127]
Dr Leaf directly quotes the work of an organisation called HeartMath for her evidence that the heart acts as a mini-brain. Dr Leaf, via Heartmath, states that:
> The heart has a network of 40,000 neurons within it, called sensory neurites, which detect circulating hormones, neurochemicals, and sense heart rate and blood pressure,
> The heart secretes “neurotransmitters” and other hormones, which have an effect on the brain, such as atrial natriuretic factor, and oxytocin,
> The heart communicates with the brain and the rest of the body through neurological, biophysical, biochemical and “energetic” (ie: electromagnetic) means [16, 17].
HeartMath clarifies, “The heart’s brain is an intricate network of several types of neurons, neurotransmitters, proteins and support cells like those found in the brain proper. Its elaborate circuitry enables it to act independently of the cranial brain – to learn, remember, and even feel and sense.” [16]
So the “evidence” looks plausible on the surface, but absurd when considered in a broader biological context. For example, my heart may have 40,000 neurons, many of which are sensitive to circulating hormones, neurochemicals and which sense and feel, but then again, so does my rectum. Does my rectum have a mini-brain as well? Clearly not. The only brain you have is the one in your cranium. We do not think with our heart, our rectum, or any other body part.
A more in-depth rebuttal of Dr Leaf’s scientific claims can be found in my book: “Hold That Thought – Reappraising the work of Dr Caroline Leaf”, via Smashwords (https://www.smashwords.com/books/view/466848) or iTunes (https://itunes.apple.com/us/book/hold-that-thought/id908877288?mt=11).
SUMMARY
The opening question from Dr Leaf’s presentation at the 2015 TEDx Oaks Christian School was, “Can the mind change the brain?”
Clearly the answer is: “No, it can not.”
Others are welcome to disagree, but in my humble opinion, I suggest that Dr Leaf is a pseudoscientist, and that her appearance on the TEDx stage is not based on scientific acumen, but on popularity and reputation, which in turn, is based on slick self-promotion and an availability cascade (a self-reinforcing process by which an idea gains plausibility through repetition).
Dr Leaf’s ideas may have popular approval, but TEDx is a vehicle for ideas worth spreading, not ideas that are popular. According to its guidelines, TEDx requests that pseudoscience be avoided, specifically stating, “TED and TEDx are platforms for showcasing and explaining genuine advances in science … Speakers should avoid the misuse of scientific language to make unsubstantiated claims.” (http://www.ted.com/participate/organize-a-local-tedx-event/before-you-start/tedx-rules)
Dr Leaf’s claims, that her research has significantly changed the lives of the students who were blessed to receive it, is simply not born out by any of her own published data – from her original case study through to her MMA project and her Switch On Your Brain program. Whatever the underlying reason … whether its hubris, naivety, or denial that’s driving her continued promotion of her own programs … her claims are baseless, and therefore an argument can be made that she breached the TEDx guidelines in presenting them, and indeed, she should never have been invited to deliver them from a TEDx stage in the first place.
The theme for the 2015 TEDx Oaks Christian School event was “Ridiculous”. I would argue that it was ridiculous that Dr Leaf promoted her research as life changing when in reality, it’s not much better than a placebo. It was ridiculous that Dr Leaf would share stories of the changes to the cognitive functioning of her patients from their brain damage and then claim that the brain does not influence the mind. It seems that Dr Leaf’s presentation certainly fitted their theme, although probably not in the way they intended. Lets hope for their sake that their “ridiculous” decision doesn’t effect their ability to host future TEDx presentations.
Of course, that’s just my opinion. What do you think, TEDx universe?
REFERENCES
- Leaf, C.M., et al., Mind-Mapping approach (MMA): a culture and language” free” technique. The South African journal of communication disorders. Die Suid-Afrikaanse tydskrif vir Kommunikasieafwykings, 1993. 40: 35
- Leaf, C.M., The Mind Mapping Approach: a model and framework for geodesic learning, in Department of Communication Pathology, Faculty of Arts1997, University of Pretoria: Pretoria. p. 266.
- Leaf, C.M., et al., The development of a model for geodesic learning: the geodesic information processing model. The South African journal of communication disorders. Die Suid-Afrikaanse tydskrif vir Kommunikasieafwykings, 1997. 44: 53
- Eppler, M.J., A comparison between concept maps, mind maps, conceptual diagrams, and visual metaphors as complementary tools for knowledge construction and sharing. Information Visualization, 2006. 5(3): 202-10
- Farrand, P., et al., The efficacy of the `mind map’ study technique. Medical Education, 2002. 36(5): 426-31 doi: 10.1046/j.1365-2923.2002.01205.x
- Wickramasinghe, A., et al., Effectiveness of mind maps as a learning tool for medical students. South East Asian Journal of Medical Education, 2007. 1(1): 30-2
- D’Antoni, A.V., et al., Does the mind map learning strategy facilitate information retrieval and critical thinking in medical students? BMC Med Educ, 2010. 10: 61 doi: 10.1186/1472-6920-10-61
- Merchie, E. and Van Keer, H., Spontaneous Mind Map use and learning from texts: The role of instruction and student characteristics. Procedia – Social and Behavioral Sciences, 2012. 69: 1387-94
- Baars, B.J., Global workspace theory of consciousness: toward a cognitive neuroscience of human experience. Progress in brain research, 2005. 150: 45-53
- Baars, B.J. and Franklin, S., An architectural model of conscious and unconscious brain functions: Global Workspace Theory and IDA. Neural Netw, 2007. 20(9): 955-61 doi: 10.1016/j.neunet.2007.09.013
- Franklin, S., et al., Conceptual Commitments of the LIDA Model of Cognition. Journal of Artificial General Intelligence, 2013. 4(2): 1-22
- Leaf, C., Who Switched Off My Brain? Controlling toxic thoughts and emotions. 2nd ed. 2009, Inprov, Ltd, Southlake, TX, USA:
- Leaf, C.M., Switch On Your Brain : The Key to Peak Happiness, Thinking, and Health. 2013, Baker Books, Grand Rapids, Michigan:
- Cohen, S., et al., Psychological stress and disease. JAMA: the journal of the American Medical Association, 2007. 298(14): 1685-7
- Lipton, B.H., The biology of belief: Unleashing the power of consciousness, matter and miracles. 2008, Hay House, Inc:
- Rosch, P. Emotional balance and health. Science of The Heart: Exploring the Role of the Heart in Human Performance – An Overview of Research Conducted by the Institute of HeartMath 2013 [cited 2013, 16/7/2013]; Available from: http://www.heartmath.org/research/science-of-the-heart/emotional-balance-health.html.
- Rosch, P. Head-Heart Interactions. Science of The Heart: Exploring the Role of the Heart in Human Performance – An Overview of Research Conducted by the Institute of HeartMath 2013 [cited 2013, October 20]; Available from: http://www.heartmath.org/research/science-of-the-heart/head-heart-interactions.html.