There are lots of medical myths that people believe.
“I have acne because I eat too much chocolate, or my face isn’t clean enough”
“Stomach ulcers are because of stress”
“I coughed up some yellow phlegm, so I must need antibiotics right?”
“My baby’s fevers are because of teething.”
Is the “chemical imbalance” theory one of them?
Dr Leaf is a communication pathologist and self-titled cognitive neuroscientist. A couple of weeks ago she opened a proverbial can of worms by quoting the out-spoken Peter Gøtzsche, claiming that psychiatric drugs are the third leading cause of death after heart disease and cancer. This did not go down well, and Dr Leaf had to issue three separate statements on social media to try and justify herself and attempt to rescue her rapidly deteriorating credibility.
Not that she issued an apology, mind you, or retracted her statement.
Today, Dr Leaf published a blog on psychiatric medications … but again, not to apologise but to further justify why she’s right, and nearly every other doctor and scientist in the world is not. Worse than that, she went so far as to accuse doctors of deliberately prescribing “clearly dangerous” drugs, which she claims have no therapeutic effects, just because of some overcooked drug-company sponsored dinner and a few pens. More on that later.
Her post is a defiant deflection, a logically flawed and factually inaccurate criticism of modern psychiatry and psychopharmacology – not fueled by research, but largely based on the books of disgruntled fringe psychiatrists and researchers with an axe to grind.
Dr Leaf doesn’t discuss the actual science of the medications that she’s so against, but simply tries to create a smokescreen of distrust.
A good example of all that is wrong with this post is contained in the opening paragraph.
Today, it has become commonplace to say that people have chemical imbalances in their brain, most notably a disruption in the proper production of dopamine (for “diseases” like ADHD) and serotonin (for “diseases” like depression). These people, it is supposed, need drugs to “cure” these chemical imbalances, hence the terms “antipsychotics” or “antidepressants”.
The first thing to note is how Dr Leaf uses the term “cure”. No doctor ever uses the word “cure”, especially when talking about complex diseases. This is a pejorative term implying that modern medicine is only interested in permanently fixing things. But it’s a straw man fallacy, a false premise that Dr Leaf then uses to cast the medical model as impotent and futile. Nice try, but no one in medicine ever promises cure, and no doctor in their right mind would ever be so narrow-minded as to suggest that drugs are the only treatment for every condition. That doesn’t mean that drugs aren’t useful, nor that the medical model is broken. As we’ll discuss soon, medications are extremely helpful for certain conditions, when used carefully, as are non-drug treatments like CBT.
Dr Leaf also puts inverted commas around the word “diseases” as if to suggest that ADHD and depression aren’t diseases, an act which smacks of petulance and willful ignorance, and is insulting to those who have or who have ever suffered from ADHD and depression. Last week, Dr Leaf was happy to share that her eldest daughter suffered from bulimia and depression, but now she’s suggesting that depression isn’t really a disease. So what is it then? Malingering? Personal weakness? Bad parenting?
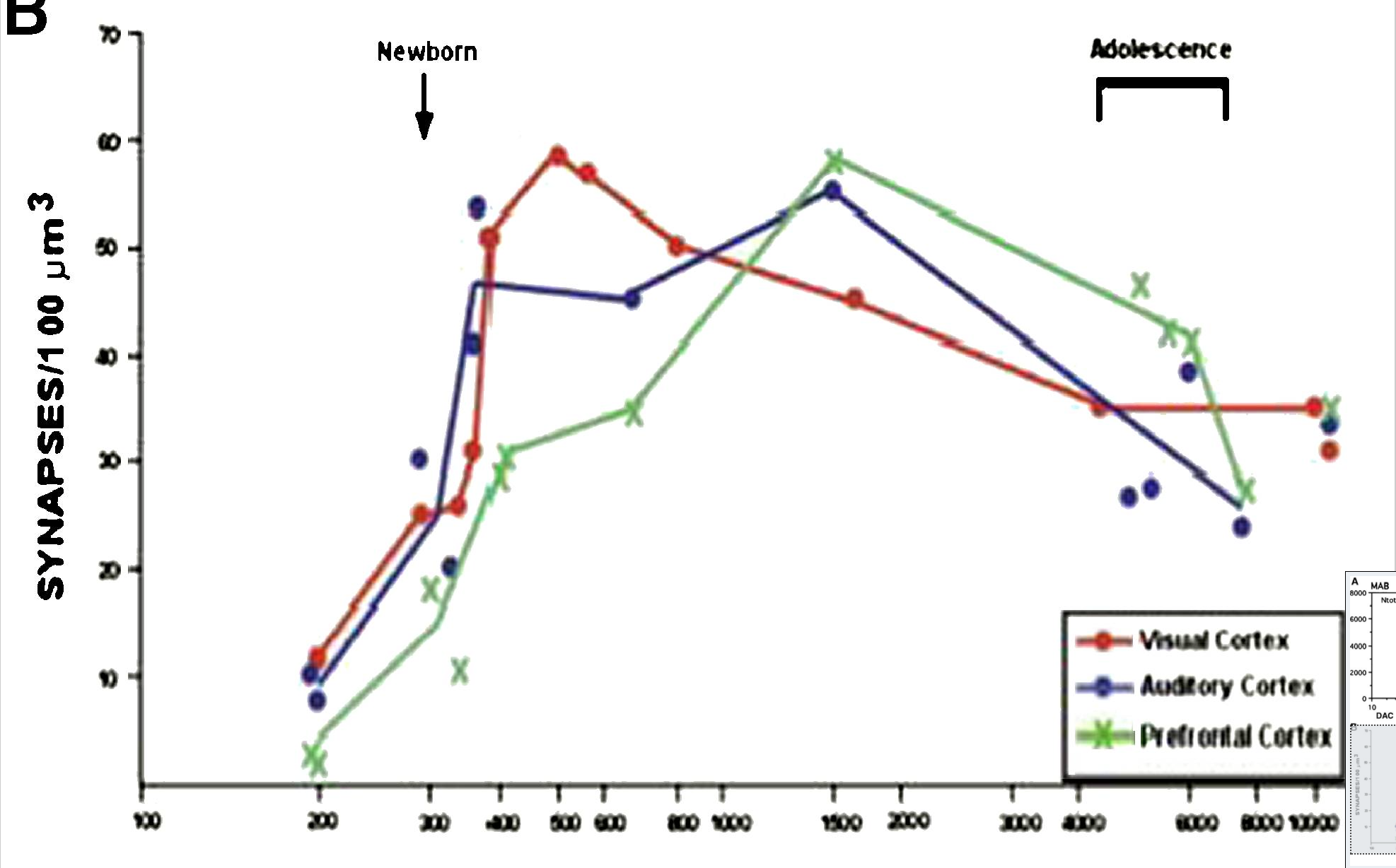
It’s really surprising that someone claiming to be a cognitive neuroscientist would ignore strong scientific evidence. For example, ADHD is associated with dopamine dysfunction as well as the dysfunction a number of other neurotransmitters [1-3]. And depression is associated with a decrease in the growth factor BDNF, (known as the neurotrophic hypothesis of depression) [4-6]. Schizophrenia, which Dr Leaf conveniently failed to mention, is clearly related to dopamine dysfunction in nerve cells of the pre-frontal cortex and the striatum, two parts of the brain that are incredibly important for how your brain processes incoming and outgoing signals [7-9].
There’s nothing to suppose here .. there’s ample evidence that psychiatric diseases are related to dysfunction within the brain, commonly with the function of neurotransmitters among other things. Call it whatever you like, the truth doesn’t change. “Chemical imbalance” is just an easy phrase for the general public to remember.
Dr Leaf then tries to suggest that psychiatric drugs don’t fix chemical imbalances but create them, citing the 1950’s observations of French researchers Deniker and Delay who noted that the first anti-psychotic, chlorpromazine, caused symptoms of Parkinson’s Disease. And indeed it did, but this wasn’t a new disease, just evidence that it worked.
Psychosis, a pathological state involving hallucinations and delusions, is because of an excess of the neurotransmitter called dopamine. Dopamine is the neurotransmitter that’s used by the nerve cells deep in the brain in a part called the basal ganglia, which acts like a central mail delivery centre for incoming and outgoing signals from other parts of the brain. The function of the nerves in one part of the basal ganglia are responsible for sending sensory signals to the frontal lobes of the brain. In another part, the signals are important for smooth movements of our muscles. Proper function depends on just the right amount of dopamine – too much and you get psychosis. Not enough and you get Parkinson’s disease symptoms.
The French researchers were simply noting the side-effects of too much medication blocking the action of dopamine in the basal ganglia – the psychosis had improved, but the blockade of dopamine was just too much in some patients, who had the opposite symptoms.
Again, Dr Leaf’s position is diametrically opposed to the published science [10, 11], and if anything, her claim contradicts her fundamental argument. After all, if chemical imbalances are myths, then how can chlorpromazine create a “new neurological syndrome” because of a chemical imbalance?
Dr Leaf then launches into a discussion on the history of the DSM and psychiatric medications. This is just the first in her ad hominem attacks on the medical profession – playing the man, not the ball if you will. If she can discredit the doctors that prescribe the medication, then she indirectly discredits the medications. This appears desperate and ultimately serves to weaken her case.
“It was just assumed that since these drugs affected brain chemistry in a certain way, the opposite reaction must be the result of the disease, notwithstanding the fact that this has never been adequately proven.”
The history of medicine is littered with cures being found without the disease being fully understood. Take Edward Jenner, for example, who is the founder of the modern technique of vaccination. He didn’t know why his smallpox vaccine worked, only that it did. Electron microscopes and a modern understanding of the immune system were centuries away, but Jenner saved billions of lives through his observation that prior vaccination with a small sample of cowpox virus would protect against smallpox [12].
When amphetamines, known to increase dopamine concentrations in the brain, caused psychotic symptoms and reserpine, a dopamine blocker, improved psychosis, it stood to reason that dopamine was a good candidate as a cause of psychosis and schizophrenia. Decades of research have gone on to further confirm and delineate the link [7]. Again, this is not “an overly simplistic explanation of chemical imbalances”. It is well proven, and rather complex.
Dr Leaf also makes the astounding accusation that psychiatrists inflicted suffering and caused “a public health disaster” by creating the DSM. The DSM, the ‘Diagnostic and Statistical Manual’ is an agreed-upon standard classification for psychiatric diagnoses. It is nothing more than a system of classification. It allows psychiatrists and researchers to speak a common language and attempt some coherence among their diagnoses.
Dr Leaf wrote, “… institutions like the American Psychiatric Association and the DSM would define what is normal, in turn telling us what it means to suffer and, essentially, what it means to be human. They medicalized misery, and today millions are suffering because of their actions, creating a public health disaster.”
That’s like saying that classifying the different types of cancer causes cancer. And that millions of people are suffering from cancer because doctors know to call it ‘cancer’. People have been suffering long before the DSM came along. The DSM doesn’t tell people they’re suffering, and it certainly doesn’t define what it is to be human. Such statements are disingenuous and melodramatic.
But wait, there’s more. “Today a psychiatrist can be praised for drugging a depressed person with mind-altering substances and, if these do not work, institutionalizing them and shocking their brain with ECT (electroconvulsive therapy). It is even an acceptable and commonplace practice to imprison mentally ill persons, drug them and lock them in solitary confinement, compelling them to live their days marinating in their own excrement.”
Dr Leaf is again playing to the fears of the public who have watched too many movies and only think of ‘One Flew Over the Cuckoo’s Nest’, ‘Shutter Island’ or scenes from ’12 Monkeys’. There are more oversight boards and lawyers than there are psychiatric patients, and the only people who are institutionalised are those who are clearly a danger to themselves or others. And while institutionalised, they are not subjected to random bouts of electrical shock as if some doctor is wandering around with a medical grade cattle prod, zapping people and laughing maniacally. Nor is anyone locked in solitary confinement and forced “to live their days marinating in their own excrement”.
The paranoid accusations continue some more. Dr Leaf accuses all psychiatrists of ignorance, and then accuses primary care physicians of negligence, by claiming that we prescribe medications that we do not understand because of the bribes and a pretty smile from a pharmaceutical rep.
Again, Dr Leaf contradicts her own argument:
Despite the recognition amongst many psychiatrists and medical health professionals that the chemical imbalance theory is not valid, drug companies like Eli Lilly still claim that ‘antipsychotic medicines are believed to work by balancing the chemical found naturally in the brain’.
Except that antipsychotic medications DO balance the naturally occurring chemical in the brain (dopamine) as we discussed earlier. What the … a drug company telling doctors how their drug works! How dare they tell the truth!
I find it disturbing that Dr Leaf would stoop so low as to insult the entire medical profession, especially every GP and family physician the world over.
Hey, I’m not above criticism. It’s important to have a good long look at ourselves from time to time, to review our practice, and make sure we’re treating our patients in the best possible way. The RACGP, the peak body of Australian GP’s, invited Prof Gøtzsche to present his opinions on anti-depressant medications so that GP’s could decide for themselves if they should adjust their prescribing.
But to suggest that primary care physicians are stupid, ignorant, incompetent and money hungry … that we would sell our soul for a drug company branded pen … is insulting. Though the irony of her statement, “we do not ask ourselves if these doctors really understand all the implications of using these substances. Not even the psychiatrists understand these drugs” is clearly lost on Dr Leaf. It’s certainly clear from the rest of her essay that Dr Leaf has no idea how these medications work or what benefits they have for those who suffer from mental ill-health.
There’s a lot more to discuss in response to Dr Leaf’s diatribe, but for the sake of brevity, I’ll try and discuss just a couple of other important themes.
Dr Leaf continues to try to make the medications sound useless and poisonous. She has several paragraphs on the placebo effect, making the false argument that the effect of the medications is just because someone tells you it will work. Of course, the placebo effect is part of the therapeutic effect, but that’s the same for all treatments, even Dr Leaf’s programs … “So, if the pastor or cell-group leader says that these programs are safe and will fix your toxic thinking, even though they get most of their information from the author, we believe wholeheartedly in what he or she may say and are more inclined to believe the program will work for us. These beliefs, which ignore actual scientific results, are buttressed by a flood of distorted and biased news reports, press releases and scientific journal articles on supposed toxic thoughts, and have transformed the theory into church dogma. So, obviously, if we experience negative side effects and do not feel the program is working, it must be something wrong with us, not the program.” Is that a fair statement?
Dr Leaf then plays the fear card again by listing all of the potential side effects from psychiatric medications. Dr Leaf is right in saying that psychiatric medications have serious proven long term side effects, and we should be careful.
For instance, if you knew that thrombocytopenia, anaphylaxis, cutaneous hypersensitivity reactions including skin rashes, angioedema and Stevens Johnson syndrome, bronchospasm and hepatic dysfunction were the potential side effects for a medication, would you take it? Most people wouldn’t. Reading the list makes that drug sound really dangerous. We should be up in arms about such a potentially harmful drug being put up for sale … except that this list of side effects isn’t a psychiatric drug at all, but’s actually the side effect profile of paracetamol (acetaminophen in the US). People take paracetamol all the time without even thinking about it.
Saying that we shouldn’t take medications because of potential side effects is a scarecrow argument, a scary sounding straw man fallacy. All drugs have serious proven long term side effects. Licencing and prescribing a medication depends on the overall balance of the good and the harm that a medication does. And no one has ever hidden these side effects from the public as if there is a giant conspiracy from the doctors and the pharmaceutical companies. They’re right there in the product information (here is the product information for fluoxetine. See for yourself).
Whilst it’s true that these side effects do happen, we know that they happen infrequently, just like we know that people win lotteries infrequently. Even so, the medications are not just doled out like sweets at a candy store. You require a minimum of ten years of university level education to be able to prescribe them.
Patients ALWAYS have a right to ask questions about possible benefits and side effects, and in my practice, I tell my patients the pros and the cons before prescribing, and I give them the choice of whether they want them or not. No one is ever forced into taking them.
Finally, Dr Leaf makes a number of irrational statements and flawed arguments in her final page of ranting. Let me quickly go through some of the honourable mentions:
* “Most people recover from depression without antidepressants” – true, because most cases of depression are mild. That doesn’t mean to say that antidepressants shouldn’t be used for severe depression, just like most people recover from upper respiratory infections without antibiotics, but that doesn’t mean that we shouldn’t use antibiotics for severe tonsillitis or pneumonia.
* “Antidepressants are no better than placebos” – It’s a controversial topic right now. There are many pushing the barrow that SSRI medications are no better than a sugar pill. But Dr Leaf has conveniently ignored several Cochrane reviews (the best of medical evidence) that shows anti-depressants work for a variety of disorders [13-15], but that psychological therapy might not [16].
* Equating antidepressants and antipsychotics with illicit drugs, and claiming that “more people die from overdoses of psychiatric drugs than illicit drugs” – This is Reductio ad absurdum – the logical conclusion from this argument is that illicit drugs are safer than psychiatric drugs. And therefore we should not give people psychiatric drugs since we don’t give people the ‘safer’ illicit drugs. But that conclusion is absurd, and when you think about it, the whole thing is based on hidden false premises – people rarely die of illicit drug overdoses because they’re illegal and are hard to come by. And also, people who use illicit drugs are not usually suicidal, whereas those given psychiatric medications sometimes are suicidal, and sometimes use them to try and commit suicide. But modern psychiatric drugs are much less dangerous in overdose than their old counterparts. It should also be noted here that more overdose suicide attempts are with paracetamol or ibuprofen than with psychiatric medications [19], but I don’t see paracetamol or ibuprofen being demonised.
* Psychiatric medications are part of a neo-liberal capitalist plot to keep the rich, richer and the poor, poorer – To me, this looks like Dr Leaf clutching at straws. Her statement, “By emphasizing that the problem lies within an individual’s biology, we are less inclined to look at their experiences and the social context of why they are feeling the way they feel. We look at the mythical chemical imbalance instead of economic exploitation, violence and inept political structures” is false. Schizophrenia is often seriously discussed in terms of neurodevelopment and not just ‘chemical imbalances’ [17, 18]. So it’s just plain wrong to suggest that researchers don’t look at the “economic exploitation, violence and inept political structures”. Oh, and Dr Leaf suggests that foster children are abused because they’re all forced to take psychiatric medication, and implies that ADHD children are abused by being force-fed Ritalin because they “move a lot in class”. Again, these are emotional over-generalisations that have no basis in reality.
Dr Leaf seems lost. She’s ignored solid published medical and scientific evidence in coming to an opinion based on the discontented rumblings of a few vocal but outspoken critics. In order to make her arguments, she has had to resort to borderline-slanderous ad hominem attacks on scientists and the medical profession, and purely emotional arguments based on fear and mistrust.
And this was only part one. If Dr Leaf’s promised second part is anything like the first, we’re in for a real treat.
Though as if that wasn’t enough, by suggesting that psychiatric drugs cause changes in your brain, cause chemical imbalances, and cause that slew of negative side effects, Dr Leaf is admitting that it’s your brain that changes your thought life, which directly contradicts her most recent teachings. After all, if thought was the dominant force in your neurology and your mind controlled your brain, then the medications would have no effect since they’re physical and aren’t connected to our mind.
So which is it? Because if the brain controls our mind, then her best-seller needs to be pulped and refunds offered to the hundred of thousands of people who bought it. But on the other hand, if the mind really does control the brain, then her entire argument against psychiatric medications implodes.
Dr Leaf has painted herself into a corner and there’s still part two to come.
References
[1] Prince J. Catecholamine dysfunction in attention-deficit/hyperactivity disorder: an update. J Clin Psychopharmacol 2008 Jun;28(3 Suppl 2):S39-45.
[2] Del Campo N, Chamberlain SR, Sahakian BJ, Robbins TW. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biological psychiatry 2011 Jun 15;69(12):e145-57.
[3] Cortese S. The neurobiology and genetics of Attention-Deficit/Hyperactivity Disorder (ADHD): what every clinician should know. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society 2012 Sep;16(5):422-33.
[4] Haase J, Brown E. Integrating the monoamine, neurotrophin and cytokine hypotheses of depression–a central role for the serotonin transporter? Pharmacol Ther 2015 Mar;147:1-11.
[5] Bus BA, Molendijk ML, Tendolkar I, et al. Chronic depression is associated with a pronounced decrease in serum brain-derived neurotrophic factor over time. Molecular psychiatry 2015 May;20(5):602-8.
[6] Sousa CN, Meneses LN, Vasconcelos GS, et al. Reversal of corticosterone-induced BDNF alterations by the natural antioxidant alpha-lipoic acid alone and combined with desvenlafaxine: Emphasis on the neurotrophic hypothesis of depression. Psychiatry research 2015 Sep 1.
[7] Howes OD, Fusar-Poli P, Bloomfield M, Selvaraj S, McGuire P. From the prodrome to chronic schizophrenia: the neurobiology underlying psychotic symptoms and cognitive impairments. Curr Pharm Des 2012;18(4):459-65.
[8] Williams GV, Castner SA. Under the curve: critical issues for elucidating D1 receptor function in working memory. Neuroscience 2006 Apr 28;139(1):263-76.
[9] Der-Avakian A, Markou A. The neurobiology of anhedonia and other reward-related deficits. Trends Neurosci 2012 Jan;35(1):68-77.
[10] Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis. Lancet 2012 Jun 2;379(9831):2063-71.
[11] Torniainen M, Mittendorfer-Rutz E, Tanskanen A, et al. Antipsychotic treatment and mortality in schizophrenia. Schizophrenia bulletin 2015 May;41(3):656-63.
[12] Riedel S. Edward Jenner and the history of smallpox and vaccination. Proc (Bayl Univ Med Cent) 2005 Jan;18(1):21-5.
[13] Arroll B, Elley CR, Fishman T, et al. Antidepressants versus placebo for depression in primary care. The Cochrane database of systematic reviews 2009(3):CD007954.
[14] Soomro GM, Altman D, Rajagopal S, Oakley-Browne M. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). The Cochrane database of systematic reviews 2008(1):CD001765.
[15] Kapczinski F, Lima MS, Souza JS, Schmitt R. Antidepressants for generalized anxiety disorder. The Cochrane database of systematic reviews 2003(2):CD003592.
[16] Jakobsen JC, Lindschou Hansen J, Storebo OJ, Simonsen E, Gluud C. The effects of cognitive therapy versus ‘treatment as usual’ in patients with major depressive disorder. PloS one 2011;6(8):e22890.
[17] van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, Krabbendam L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychological medicine 2009 Feb;39(2):179-95.
[18] Howes OD, Murray RM. Schizophrenia: an integrated sociodevelopmental-cognitive model. Lancet 2014 May 10;383(9929):1677-87.
[19] Prescott K, Stratton R, Freyer A, Hall I, Le Jeune I. Detailed analyses of self-poisoning episodes presenting to a large regional teaching hospital in the UK. Br J Clin Pharmacol 2009 Aug;68(2):260-8.
Disclaimer
- Do not abruptly stop any medications that you are taking. Talk to your licenced physician first. They’re not all money-hungry, imbecilic drug-company bitches. Most of them actually know what they’re talking about.
- For the record, I declare that I have no connection with any pharmaceutical company. I do not accept gratuities of any form from any sales representative. I don’t eat their food, I don’t take their pens, and I don’t listen to their sales pitches
Update – 8 August 2016.
Dr Leaf has since taken the offending post from her blog page, and re-gifted it as an answer on her “Scientific” FAQ page (“Chemical Imbalances and Mental Health” http://drleaf.com/about/scientific-faqs/). It remains as unbalanced and inaccurate as it’s former iteration. It’s unfortunate that Dr Leaf continues to make such preposterous claims in the face of overwhelming scientific evidence to the contrary.