
We’ve all heard of being “homesick”, or “heartsick”, or “lovesick”. Sometimes when we’re extremely sad, we feel the knot in our stomachs, the pressure in our chests, or the confusion and distraction in our minds as the waves of sadness wash over and discombobulate us.
But can being sad really make you physically ill as well as emotionally distraught?
Dr Caroline Leaf declared today on her social media platforms that “Feeling sad can alter levels of stress-related opioids in the brain and increase levels of inflammatory proteins in the blood that are linked to increased risk of comorbid diseases including heart disease, stroke and metabolic syndrome.”
Dr Caroline Leaf is a communication pathologist and a self-titled cognitive neuroscientist. She believes that our cognitive stream of thought determines our physical and mental health, and can even influence physical matter through the power of our minds.
She also added some further interpretation to her meme: “So this is more evidence that our thoughts do count: they have major epigenetic effects on the brain and body! We need to apply the principles in the Bible and listen to the Holy Spirit – no excuses this year!”
With all due respect to Dr Leaf, the study she quotes doesn’t prove anything of the sort.
Dr Leaf’s meme is a copy and paste of the opening paragraph of a news report published by the university’s PR people to promote their faculty. This isn’t a scientific summary, it’s a hook to draw attention to an article which amounts to a PR puff piece. If Dr Leaf had read further into the article, I don’t think she would have been quite so bold in claiming what she did.
The article discussed a study by Prossin and colleagues, published in Molecular Psychiatry [1]. You can read the original study here. The study specifically measured the change in the level of the activity of the opioid neurotransmitter system and the amount of a pro-inflammatory cytokine IL-18 across two experimental mood states, and in two different groups of volunteers, people with depression, and those without.
For a start, it’s important to note that the study isn’t referring to normal day-to-day sadness. This was an experimentally induced condition in which a sad memory was rehearsed so that the same feeling could be reproduced in a scanner, and the study was looking at the effect of this sad “mood” on people who were pathologically sad, that is, people diagnosed with major depression.
It’s well known that people with depression are at a higher risk of major illnesses, such as heart attacks, strokes and diabetes [2] The current study by Prossin et al looked experimentally at one possible link in the chain, a link between a neurotransmitter system that’s thought to change with emotional states, and one of the chemical mediators of inflammation.
They found that:
> Depressed people were much sadder to start with, and remained so throughout the different conditions. The depressed people stayed sadder in the ‘neutral’ phase, and the healthy cohort couldn’t catch them in the ‘sad’ phase.
> Depressed people had a much higher level of the inflammatory marker to start with, and interestingly, this level dropped significantly with the induction of the neutral phase and the sad phase. What was also interesting was that the level of the inflammatory marker was about the same in the baseline and the sad phase for the healthy volunteers.
> A completely different pattern of neurotransmitter release was seen in the two different groups. People with depression had an increase in the neurotransmitter release over a large number of areas of the brain, whereas in the healthy controls with normal mood, the sad state actually resulted in a decreased amount of neurotransmitter release, and in a much smaller area within the brain. This suggests that the opioid neurotransmitter system in the brains of depressed people is dysfunctional.
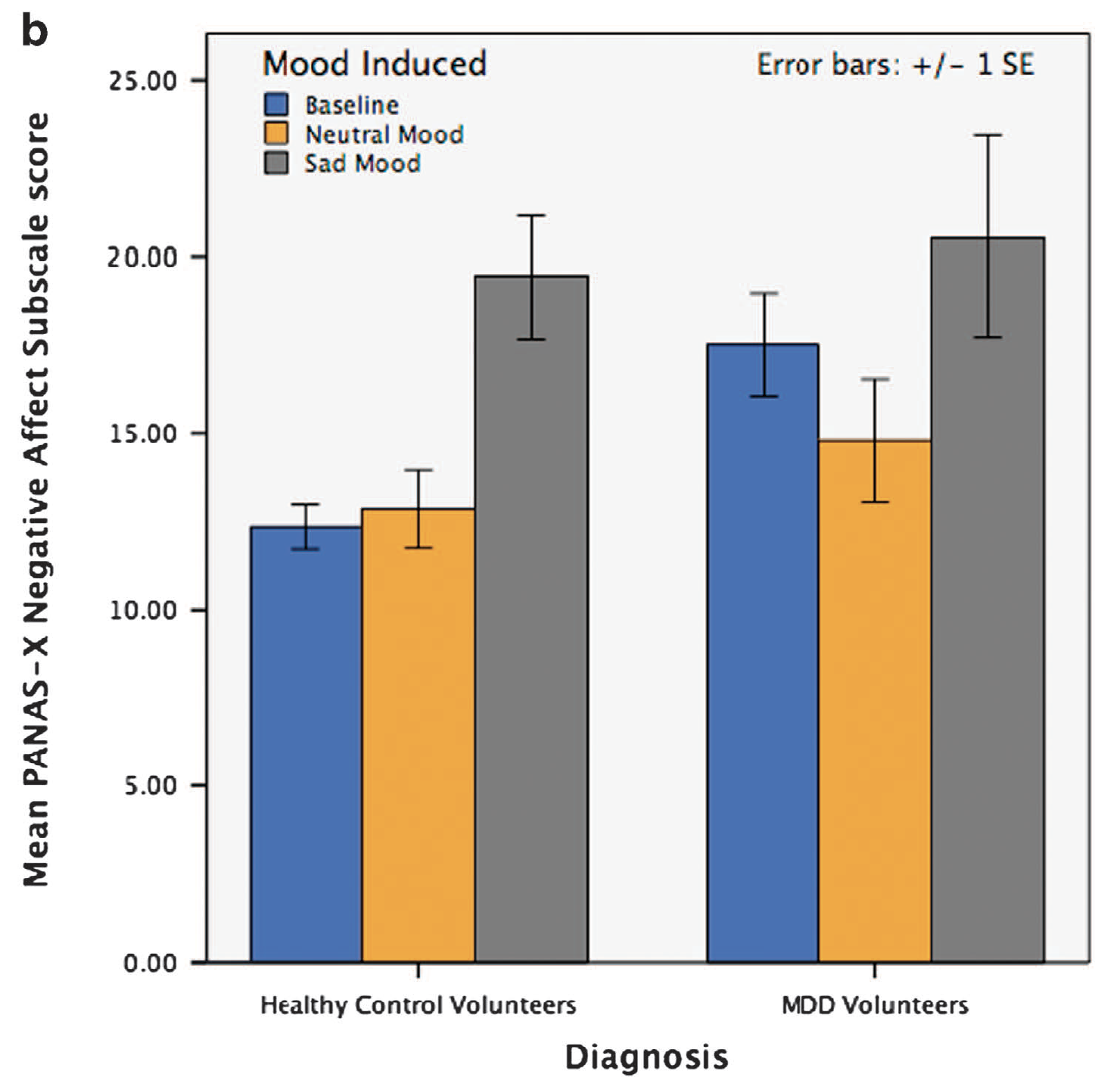
Affect/Sadness Scores – Prossin et al Molecular psychiatry 2015 Aug 18.
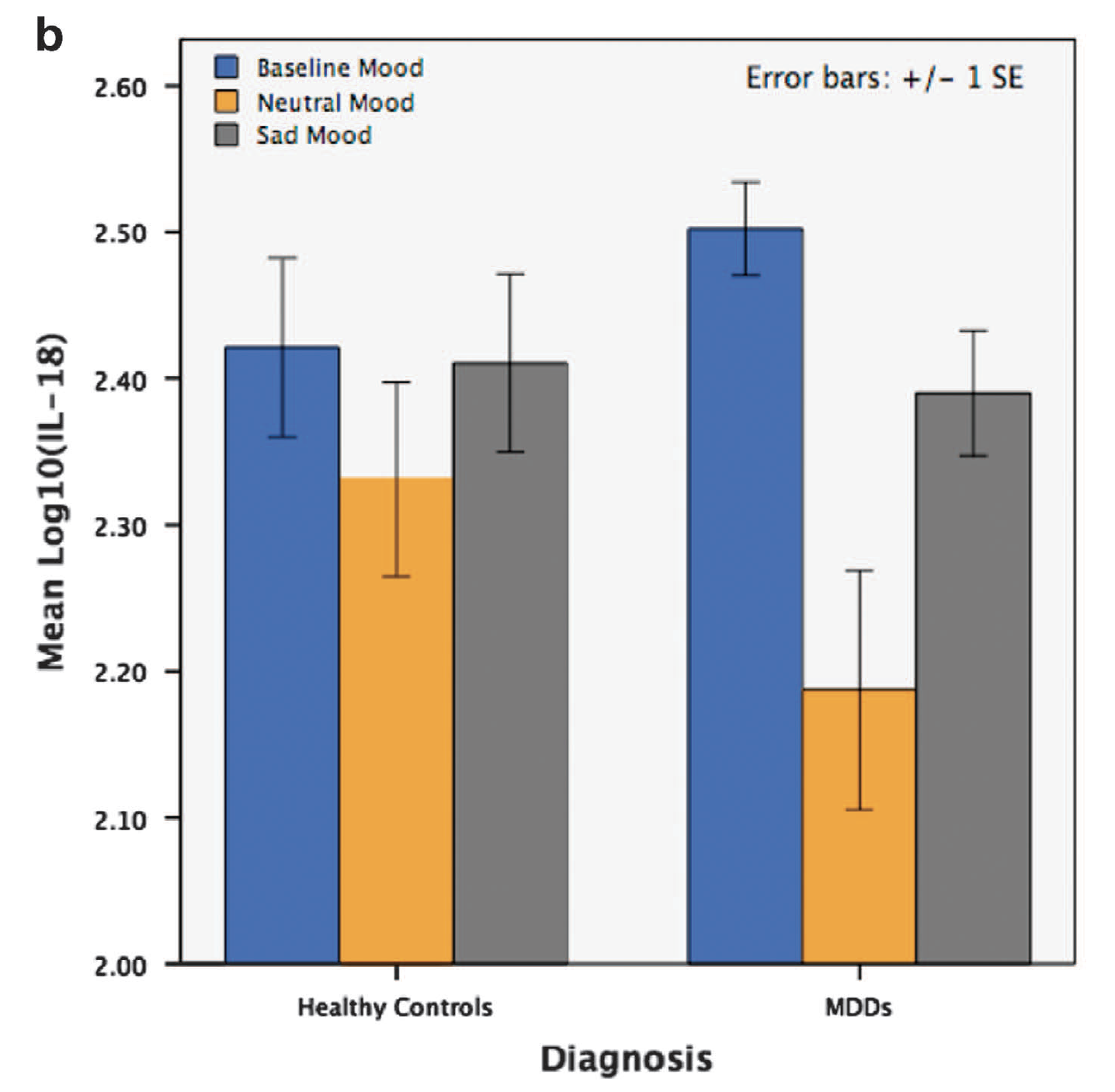
IL18 v Mood state/diagnosis – Prossin et al Molecular psychiatry 2015 Aug 18.
Effectively, the results of the study reflect what’s already known – the emotional dysregulation seen in people with depression is because of an underlying problem with the brain, not the other way around. And, sadness in normal people is not associated with a significant change in the evil pro-inflammatory cytokine.
So, according to Prossin’s article,
- normal sadness in normal people is not associated with physical illnesses.
- sadness is abnormally processed in people who are depressed, which maybe related to an abnormal inflammatory response, which might explain the known link between depression and increased risk of illness
The article is not “more evidence that our thoughts do count.” If anything, it shows that underlying biological processes are responsible for our thoughts and emotions and their downstream effects, not the thoughts and emotions themselves.
And unfortunately, it appears that Dr Leaf hasn’t got past the opening paragraph of a puff piece article before jumping to a conclusion which only fits her worldview, not the actual science.
References
[1] Prossin AR, Koch AE, Campbell PL, Barichello T, Zalcman SS, Zubieta JK. Acute experimental changes in mood state regulate immune function in relation to central opioid neurotransmission: a model of human CNS-peripheral inflammatory interaction. Molecular psychiatry 2015 Aug 18.
[2] Clarke DM, Currie KC. Depression, anxiety and their relationship with chronic diseases: a review of the epidemiology, risk and treatment evidence. Med J Aust 2009 Apr 6;190(7 Suppl):S54-60.
