Dr Caroline Leaf is a communication pathologist and a self-titled cognitive neuroscientist. She also likes to think that she’s an expert on mental health. So this morning, she felt like she was quite justified in publishing a meme about the evils of psychiatric medications.
She quoted Professor Peter Gøtzsche, stating that “Psychiatric Drugs are the third leading cause of death, after heart disease and cancer.” Then followed it with “Take all thoughts into captivity, not drug all thoughts into captivity. You have the mind of Christ! (1 Cor 2:16) **DRUG WITHDRAWAL should ALWAYS be done under the supervision of a qualified professional. These drugs alter your brain chemistry, and withdrawal can be a difficult process.”
The subsequent comments were primarily made up of the usual sycophantic responses that Dr Leaf has cultivated by blocking anyone that disagrees with her. But there were more than the usual responses confused by her meme, and quite a few that we’re asking for help in weaning off the medications that they were on.
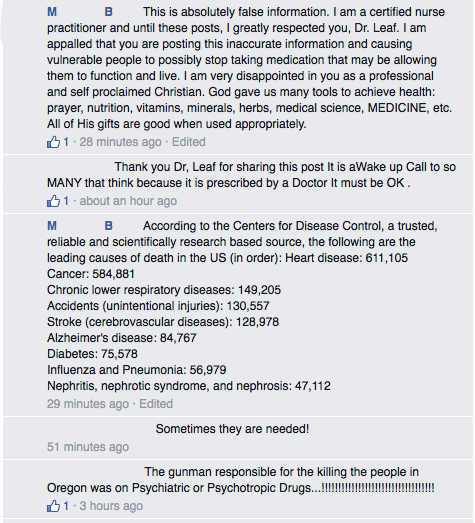
Then there were those who weren’t happy at all. One respondent, a certified Nurse Practitioner, wrote, “I am appalled that you are posting this inaccurate information and causing vulnerable people to possibly stop taking medication that may be allowing them to function and live.” The same person followed up with another comment soon after, quoting the CDC figures for the top ten causes of death in the US, in which the third on the list wasn’t psychiatric drugs at all, but chronic lower respiratory diseases.
The overall response must have taken her aback, because Dr Leaf posted a follow-up comment to explain herself, an unusual step for her.
In it, she said, “I do not speak out against psychiatric medication because I want to condemn people, or make them feel guilty. I want to help people. If, for example, I knew that eating some food could kill you or seriously injure you, and kept this to myself, you would justifiably be angry at me. These drugs have serious, proven long term side affects that are hidden from the public, and the logic behind them is not God’s desire for you to be healthy in your spirit, soul and body. Psychiatric drugs are based off of a theoretical view of evolution as a mindless, unguided process that created you as mechanistic individual with a biological brain that has chemicals that need to be “balanced”. You are more than your biology; you are the temple of the Lord, created in his image. This is not a game: these drugs can decrease your lifespan by 15-25 years. I want you to have those 15-25 years, and I want them to be characterized by God’s perfect, good plan for your life. I ask you to not to just take my word for this, but to do your own research. You can find a multitude of references on my site http://www.drleaf.com under Scientific FAQs. It is my earnest desire that people do not perish for lack of knowledge (Hosea 4:6). **DRUG WITHDRAWAL should ALWAYS be done under the supervision of a qualified professional. These drugs alter your brain chemistry, and withdrawal can be a difficult process.”
But it was too late. Dr Leaf had opened a can of worms, and once out, those wriggly little critters are impossible to put back in.
Both her initial offering and her reply shows just how poor Dr Leaf’s understanding of mental health truly is. She is fixated on the notion that the mind controls the brain, and she is unwilling to consider any other notion, instead preferring to accept any opinion that conforms to her world view, no matter how poorly conceived it might be. This includes the work of Gøtzsche, accepting it as gospel even though he has critics of his own.
It’s important to examine Dr Leaf’s reply in more detail as her statement has the potential to cause a great deal of harm to those who are the most vulnerable. Lets break down Dr Leaf’s statement and review each piece, and then I will outline some other important and contradictory considerations of Dr Leaf’s stance.
- The safety of psychiatric medications
Dr Leaf claims that “These drugs have serious, proven long term side affects {sic} that are hidden from the public” and “This is not a game: these drugs can decrease your lifespan by 15-25 years.”
Dr Leaf is right in saying that psychiatric medications have serious proven long term side effects. And we should be careful. I mean, if you knew that thrombocytopenia, anaphylaxis, cutaneous hypersensitivity reactions including skin rashes, angioedema and Stevens Johnson syndrome, bronchospasm and hepatic dysfunction were the potential side effects for a medication, would you take it?
Most people wouldn’t. Reading the list makes that drug sound really dangerous. We should be up in arms about such a dangerous drug … except that this list of side effects isn’t for a psychiatric drug at all, but is actually the side effect profile of paracetamol (Panadol if you’re in Australia, Tylenol if you’re in the US). People take paracetamol all the time without even thinking about it. Saying that we shouldn’t take medications because of potential side effects is a scarecrow argument, a scary sounding straw man fallacy. All drugs have serious proven long term side effects, and most of the time, those serious long term side effects don’t occur. Licensing and prescribing a medication depends on the overall balance of the good and the risk of harm that a medication does.
Oh, and no one has ever hidden these side effects from the public as if there’s some giant conspiracy from the doctors and the pharmaceutical companies. The side effects are listed right there in the product information (here is the product information for fluoxetine. See for yourself).
As for Dr Leaf’s assertion that psychiatric medications decrease your lifespan by 10-25 years, I think that’s a red herring. I read through Dr Leaf’s ‘Scientific FAQ’ and I couldn’t find any references that back up these statements, so who knows where she got this figure of ’15-25 years’ from.
On the contrary, what is known is that severe mental illness is associated with a 2 to 3-fold increase in mortality, which translates to an approximately 10-25 year shortening of the lifespan of those afflicted with severe depression, schizophrenia or bipolar disorder [1]. So Dr Leaf has it backwards. It isn’t the medications that cause people who take them to die 25 years earlier than they would have without the illness, but it’s the illness itself.
- The benefits of long term psychiatric medications
So psychiatric medications have their side effects, true, but they also have protective benefits which Dr Leaf consistently fails to acknowledge.
Correll and colleagues note in the conclusion to their article that “Although antipsychotics have the greatest potential to adversely affect physical health, it is important to note that several large, nationwide studies providing generalizable data have suggested that all-cause mortality is higher in patients with schizophrenia not receiving antipsychotics.” [1]
More specifically, in one recent study, the use of any anti-psychotic medication for a patient with schizophrenia decreased their mortality by nearly 20% [2]. In another study, the mortality of those with schizophrenia who did not take anti-psychotics was nearly ten times that of the healthy population, but taking anti-psychotic medication cut that back to only four times the risk [3].
These findings are mirrored by other studies on other psychiatric medications. For example, as noted by Correll and colleagues, “clozapine, antidepressants, and lithium, as well as antiepileptics, are associated with reduced mortality from suicide. Thus, the potential risks of antipsychotics, antidepressants and mood stabilizers need to be weighed against the risk of the psychiatric disorders for which they are used and the lasting potential benefits that these medications can produce.” [1]
So psychiatric medications are not useless. Let me be clear, I’m not saying that taking psychiatric medications always makes life a cake-walk – there are still side effects from the medications, and the disease isn’t always fully controlled. But on average, well treated patients with psychiatric conditions clearly do better than patients who are not treated.
Therefore Dr Leaf’s assertion that psychiatric medications are harmful are inaccurate. And given that there are genuine benefits to these medications, particularly in the prevention of suicide, Dr Leaf’s discouragement of these medications has the real potential to result in real harm to those of her followers who take her at her word.
- The ‘logic’ behind psychiatric medications
Dr Leaf says in her statement, “the logic behind them (psychiatric medications) is not God’s desire for you to be healthy in your spirit, soul and body. Psychiatric drugs are based off of a theoretical view of evolution as a mindless, unguided process that created you as mechanistic individual with a biological brain that has chemicals that need to be ‘balanced’. You are more than your biology; you are the temple of the Lord, created in his image.”
Dr Leaf’s argument here is that based on a false premise and some straw man fallacies which inevitably leads to a false conclusion.
Evolution is a mindless unguided process
Evolution says that you are just a machine
Psychiatric illness is because of a chemical imbalance in that machine (a false premise)therefore taking psychiatric medication is accepting evolution (a straw man fallacy)
and
You are more than your biology,
you are the temple of the Lord, created in his image,therefore evolution is wrong (another straw man fallacy)
therefore psychiatric medications are not God’s desire (false conclusion)
The problem with this logic is that it could be applied to all medications, since modern medicine has predominantly been devised by agnostic scientists within an evolutionary framework, and nearly all disease is defined by an imbalance of one thing or another.
For example, simply rewording Dr Leaf’s statement shows up the distorted logic that it entails:
“Insulin can have serious, proven long term side affects that are hidden from the public, and the logic behind it is not God’s desire for you to be healthy in your spirit, soul and body. Diabetes is based off of a theoretical view of evolution as a mindless, unguided process that created you as mechanistic individual with a biological pancreas that has chemicals that need to be ‘balanced’.”
You can’t have this both ways. If psychiatric medications are against God’s plan, then all medications are against God’s plan. But if we accept medications for physical ailments, then we also have to accept medications for psychological ailments.
- The Mind-Brain link
Dr Leaf tried to protect herself with a glib disclaimer at the end of both posts in question today, “**DRUG WITHDRAWAL should ALWAYS be done under the supervision of a qualified professional. These drugs alter your brain chemistry, and withdrawal can be a difficult process.”
Which is interesting, because in her Scientific FAQ, Dr Leaf has this to say about the mind,
“The Brain is part of the Physical Body and therefore is controlled by the Mind. The Mind does not emerge from an accumulation of Brain activity. Brain activity, rather, reflects Mind activity. Even though the Mind controls the Brain, the Brain feeds back to, and influences, the Mind. The Brain seats the Mind, and therefore the Mind influences the Physical world through the Brain.”
So if that’s true, then why is withdrawal from psychiatric medication so difficult? If the mind is outside the physical realm and controls the brain as Dr Leaf proposes, then the medications effect on brain chemistry should make little or no difference to the mind, and withdrawal should be simple.
The fact that withdrawal from these medications is not simple is testament to the fact that the mind is a function of the brain, and does not control the brain as Dr Leaf proposes here and through her books and other written materials.
Issuing the warning is responsible, but shows again just how far Dr Leaf’s teaching is from scientific reality.
- Dr Leaf’s motivations
Finally, I want to talk about Dr Leaf’s motivation. In her statement, Dr Leaf said, “I do not speak out against psychiatric medication because I want to condemn people, or make them feel guilty. I want to help people.” And, “I want you to have those 15-25 years, and I want them to be characterized by God’s perfect, good plan for your life … It is my earnest desire that people do not perish for lack of knowledge (Hosea 4:6).”
I want to state, for the record, that I believe Dr Leaf when she says this. I don’t doubt her motives are to try and help people. But good intentions are not enough. What she says has real life consequences.
Dr Leaf is idolised by her followers and portrayed as a mental health expert by the churches she preaches at. People don’t question experts recommended to them by their pastors or their friends. So when she says that psychiatric medications kill people, people on psychiatric medications will want to come off them, because of fear, because of stigma, because of their desire to live true to God and his good and perfect plan. Without wanting to sound melodramatic, there is a very real chance that some of those people who were stable on their medications but who unnecessarily cease them because Dr Leaf told them to, may harm themselves or take their own life, since that’s what the studies tell us [1, 4]. At the very least, they are likely to have a shorter life expectancy because of it [2, 3]. So telling people that psychiatric medications are dangerous is morally and ethically dubious.
There are also potential legal implications too. God forbid, but if a person committed suicide because they went off their medication because of what Dr Leaf wrote, law suits could easily follow. No one wants that situation. Dr Leaf also runs the risk of being accused of practicing medicine without a licence, since some of her followers have asked personal medical questions in the comments, and the reply from Dr Leaf’s Facebook team is to direct them to their programs like the 21-day detox, which depending on the legal interpretation and the mood of a judge, could be seen as giving medical advice, which Dr Leaf is not legally qualified to give.

To summarise, I certainly hope that neither of these hypothetical scenarios becomes reality, but Dr Leaf and her social media team are skating on thin ice, and a glib disclaimer at the end of a post won’t necessarily cut it.
I would hope that Dr Leaf and her social media team would reconsider their approach. In fact, I would suggest that Dr Leaf unequivocally apologises for what she’s written, retracts her statement, and encourages people to see their doctors if they have concerns about their medication, or their mental health.
Indeed, I would implore Dr Leaf to step back and re-evaluate the entire breadth of her teaching, and the advice that she is giving. Dr Leaf is obviously a very smart woman and a very engaging speaker. With great power comes great responsibility. If she were to reconsider her teaching and start from a basis of scientific fact, then she could be a major force for the good of the church and its physical and mental health. At the moment, I fear that she is doing the opposite.
This is not a game: people’s lives are at stake. I hope that Dr Leaf sees this before it’s too late.
References
[1] Correll CU, Detraux J, De Lepeleire J, De Hert M. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World psychiatry : official journal of the World Psychiatric Association 2015 Jun;14(2):119-36.
[2] Tiihonen J, Lonnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet 2009 Aug 22;374(9690):620-7.
[3] Torniainen M, Mittendorfer-Rutz E, Tanskanen A, et al. Antipsychotic treatment and mortality in schizophrenia. Schizophrenia bulletin 2015 May;41(3):656-63.
[4] Tiihonen J, Suokas JT, Suvisaari JM, Haukka J, Korhonen P. Polypharmacy with antipsychotics, antidepressants, or benzodiazepines and mortality in schizophrenia. Archives of general psychiatry 2012 May;69(5):476-83.
Here’s my glib disclaimer: This article is a rebuttal of Dr Leaf’s opinion regarding psychiatric medication. This blog doesn’t constitute individual medical advice. If you do not like your medication or think you should come off it, please talk to your own GP or psychiatrist. Do not stop it abruptly or without adequate medical advice.